
两周前您在踢球时扭到了脚踝。X 光片显示没有骨折,您依照一般踝关节扭伤的康复方式处理,本来以为几周内就能回到训练场上。三周过去了,踝关节还是不对劲。肿胀消退了,但承重时仍有一种与一般内翻性扭伤不一样的疼痛。痛感位置较高,靠近小腿,上楼梯会更明显,跑步蹬地时最难受。这是我们诊所常见的高位踝关节扭伤早期表现,因为受伤当下看起来与普通踝关节扭伤无异、X 光在轻度案例中通常显示正常、初期所安排的康复也是一般扭伤的标准计划,所以往往在头 2 至 3 周内被忽略。等到察觉康复计划没起作用时,损伤已经被多承受了 3 至 4 周的不当负荷。
高位踝关节扭伤指的是下胫腓联合(syndesmosis)的损伤,也就是连结小腿两块骨头(胫骨与腓骨)、位于踝关节上方的强韧纤维结构。与一般急性踝关节扭伤主要影响踝关节外侧韧带不同,高位踝关节扭伤伤及的是连结两根小腿骨、位于踝关节上方的韧带。损伤机制不同、恢复时间不同、康复方式也不同;由于头 1 至 2 周看起来与一般扭伤极为相似,早期辨识出特征是避免后续 3 至 6 个月反覆波折的关键。
高位踝关节扭伤的症状
如果不熟悉高位踝关节扭伤,很容易把它的症状误以为是内翻性踝关节扭伤。但只要知道要观察什么,高位踝关节扭伤其实有它自己可辨识的症状模式。
- 疼痛位置较高,位于踝关节上方: 最明显的压痛点位于两块小腿骨之间,大约在踝关节前外侧(anterolateral)上方 2 至 3 指宽的位置。
- 蹬地与转向时疼痛加剧: 一般踝关节扭伤多在脚踝向外翻(内翻)时疼痛最明显,高位踝关节扭伤则通常在跑步、蹬地、上楼梯,以及任何快速转向时引发疼痛。
- 胫腓挤压试验可复现疼痛: 在小腿中段挤压会让踝关节出现疼痛。这是下胫腓联合损伤的临床征象,并非外侧踝关节扭伤会出现的反应。
- 背屈合并外旋试验可复现疼痛: 将脚向上勾起同时向外旋转可重现疼痛,这是我们会观察的第二个临床征象。
- 肿胀位置高于一般扭伤: 肿胀像是出现在踝关节上方的隆起,而非集中在踝关节外侧。
- 急停或前冲弓步时疼痛: 较少被提及,但突然的急停或重量前压的弓步会对下胫腓联合产生压力,引发疼痛。
我们最常向患者说明的早期辨识重点包括:疼痛位置(高于踝关节)、疼痛随蹬地出现而非随内翻出现,以及上述两项临床测试中任一项可复现疼痛。
由于损伤机制是最强且最具辨识度的线索之一,下一段就来说明高位踝关节扭伤实际上是如何发生的。
高位踝关节扭伤的成因
高位踝关节扭伤的损伤机制与一般踝关节扭伤相当不同。辨识机制本身,就是判断这不是一般内翻性损伤的第一线索。
是什么造成高位踝关节扭伤?
- 脚被牢牢踩在地面、小腿却被外旋扭转: 经典的损伤机制,在我们最常见到的足球员身上尤为常见。当腿部完全承重时,脚被强力地向外旋转。足球抢断、橄榄球冲撞,以及任何接触性运动中都很常见。
- 脚踩在地面下、踝关节被强力背屈: 例如向前跌倒、身体重量压在脚的前端时;常见于铲球、脚卡住却身体冲前的急停,或下楼梯时脚未移动但身体重心被带向前方。
- 接续在高能量的踝关节创伤之后: 在较严重的踝关节损伤中,高位踝关节扭伤常与高冲击性的外侧踝关节韧带损伤或腓骨骨折同时发生。能造成其中一项的强力机制,往往也会造成另一项。
哪些人基础风险较高?
- 足球与橄榄球运动员,接触性铲球与脚踩在地面下被旋转的力量在训练与比赛中很常出现。这是我们诊所最常见的族群。
- Hyrox 与 CrossFit 运动员,训练中包含大量负重位移、跳跃以及快速变向。
- 在不平地面上活动的登山客与越野跑者,意外的踝关节旋转在负重下更容易发生。
- 舞者与芭蕾表演者,特别是落地与旋转时。
- 国民服役人员,在体能训练中常面对障碍场地与崎岖地形。
- 任何曾有慢性踝关节扭伤或踝关节整体不稳的人,关节本身的保护反应已被削弱。
容易与高位踝关节扭伤混淆的情况
高位踝关节扭伤是常被忽略的损伤,这也是我们从患者口中常听到的情况。早期几周内有几种状况表现非常相似,正确诊断之所以重要,是因为处置方式根本上不同。
内翻性踝关节扭伤
是我们最常见的误诊。内翻性踝关节扭伤会造成踝关节外侧的疼痛与肿胀,位置与高位踝关节扭伤的疼痛区相近。虽然位置相似,疼痛模式却不同,并且可以透过特定临床测试(胫腓挤压试验与背屈合并外旋试验)加以区分。若您已经针对踝关节扭伤进行康复数周却未见改善,这就是首先需要排除的情况。
腓骨骨折
高能量的踝关节损伤可能同时造成下胫腓联合损伤与腓骨骨折。可能两者其一发生,也可能同时存在。X 光与临床检查可以将两者分辨开来。
三角韧带损伤(内侧踝关节扭伤)
内侧(三角)踝关节韧带的损伤同样源于外旋机制,与高位踝关节扭伤的机制相同,因此两者也常合并出现。区分关键在于疼痛位置与临床测试。
距骨穹窿损伤
发生在踝关节内的软骨损伤,可能源自同一种高能量机制。如果踝关节内深处出现钝痛,并伴随持续的卡住或锁住感,就要往这个方向考虑。
踝关节撞击综合征
未妥善处理的高位踝关节扭伤,长期下来常演变为前踝撞击综合征,原因在于不稳定的下胫腓联合让骨头在踝关节背屈时出现异常碰撞。原始损伤后数月仍持续存在的前踝疼痛,可能是撞击综合征而非持续的扭伤未愈。

高位踝关节扭伤的治疗与预防
高位踝关节扭伤的恢复需要分阶段进行,并给予时间保护。下胫腓联合是连结两块小腿骨的结构性关节,与踝关节外侧的韧带性质不同,未愈合前过早承受负荷会使两根骨头出现分离趋势,造成日后更难处理的慢性不稳。处置上先以受保护的承重开始,再过渡到渐进的活动度与肌力训练,最后才是运动专项性的回归。手术则保留给高度损伤、保守治疗后仍未稳定的案例。
保守治疗
- 行走靴与急性期保护: 在急性期(第 0 至 4 周),首要任务是在下胫腓联合开始愈合的同时给予保护。会使用行走靴或气垫护具,并在可耐受范围内进行受保护的承重;在头 1 至 2 周内,若疼痛剧烈,可能需要拐杖辅助。跑步、跳跃与运动须完全停止。第一周内透过冰敷、抬高,以及在医师建议下使用短期的消炎药物来控制肿胀与疼痛。
- 活动度、肌力与平衡康复: 从中期阶段(第 4 至 8 周)开始,温和的踝关节活动度训练可以开始恢复关节活动范围,同时过渡到不再使用行走靴。接着进行小腿与足部小肌群的肌力训练,再进入渐进的本体感觉与平衡训练,按照单脚平衡、小幅跳跃、直线跑步、变向训练的顺序推进。康复持续到回归运动阶段,并最好与物理治疗师协同进行。
- 踝足矫形器或支撑性护具: 踝足矫形器或支撑性护具可在下胫腓联合巩固期间限制外旋动作。通常在中期阶段引入,对高强度活动需求的患者可延续到回归运动的初期。
- 聚焦冲击波治疗与磁感应传导疗法: 若中期阶段疼痛改善停滞,聚焦冲击波治疗与磁感应传导疗法可以刺激身体本身的修复反应,并缓解发炎成分。
- 定制足部矫形鞋垫: 若生物力学因素是原始损伤的成因之一,定制足部矫形鞋垫能优化足部与踝关节的受力分布,在回归运动与日后活动中降低复发风险。
- 运动专项回归训练与护踝: 在回归活动阶段(第 8 至 16 周),运动专项性的动作训练应在重新进入身体接触前展开。以足球员为例,会从直线跑步进展到转向,再从转向进展到铲球,最后再从铲球进展到渐进的对抗性比赛。回归接触性运动初期,建议配戴护踝或贴扎至少 6 个月。
- 长期稳定度与本体感觉训练: 将踝关节稳定度与本体感觉训练纳入日常训练。穿着适合该运动的鞋款,特别是合脚且抓地良好的钉鞋。针对可能引发原始损伤机制的高风险情境,加强动作、反应与应变能力的训练。若踝关节仍存有不稳,在高冲击活动中继续使用护踝。
当保守治疗不足以处理时
手术在低度高位踝关节扭伤中并不常见,主要保留给影像上两根小腿骨之间出现明显分离的高度损伤,或在保守治疗数月后仍未稳定的案例。当需要手术时,海峡足科诊所会转介给具备下胫腓联合重建经验的骨科医师同业。多数低度案例在合适的治疗、结构化的康复与足够时间下,可以完全恢复。

海峡足科诊所为您管理高位踝关节扭伤
高位踝关节扭伤是早期准确诊断会直接影响恢复时间与结果的损伤。能在受伤后头 2 至 3 周内、还来不及造成额外损伤之前就来诊所的患者,其预后远比拖延数月才就诊的患者更佳。在海峡足科诊所,针对疑似高位踝关节扭伤的评估会聚焦在病史、临床检查,以及是否需要影像确认的明确讨论。
诊断确定后,会依损伤分级制定处置计划,可能包括行走靴或踝足矫形器的配戴、用于稳定的定制足部矫形鞋垫,以及结构化的渐进负荷康复训练。如果您已经针对踝关节扭伤康复数周仍未见改善,且疼痛位置比预期更靠近小腿上方,欢迎与我们的团队联系,或预约咨询进行评估,以处理您的高位踝关节扭伤。
关于高位踝关节扭伤的常见问题
高位踝关节扭伤需要多久才能痊愈?
低度损伤通常需要 6 至 12 周,较高度损伤则可能需要 3 至 6 个月才能充分愈合。如果加上回归特定运动(尤其是足球、橄榄球等接触性运动)所需的康复时间,时程可能更长。在下胫腓联合尚未巩固前过早承受负荷,特别是跑步、跳跃或高冲击运动,是最常见把 12 周恢复拖成 6 个月恢复的原因。延迟诊断的患者通常恢复也较慢,因为损伤在正确处置开始之前,已被不当负荷数周。
高位踝关节扭伤时还能走路吗?
可以,但需要适当保护。早期标准治疗是使用行走靴或气垫护具,并在可耐受范围内进行受保护的承重,仅在睡觉与洗澡时取下。头 1 至 2 周内若疼痛剧烈,可加入拐杖辅助。不加保护地走路会让下胫腓联合承受更多压力,造成日后更难解决的慢性不稳。急性期度过、疼痛缓解后,会建议您过渡到穿着具有支撑性的鞋款走路。
X 光可以显示高位踝关节扭伤吗?
在低度与中度高位踝关节扭伤中,X 光显示正常是很常见的。原因在于损伤位于下胫腓联合及其韧带(下胫腓前韧带),而不在骨头本身;X 光只能呈现骨头,无法呈现韧带。然而,若下胫腓联合损伤属于较高度,X 光可能显示胫骨与腓骨之间的间距变宽,但前提是您的临床医师有指定正确的踝关节 X 光投照角度。诊断上更敏感的影像选项是 MRI。
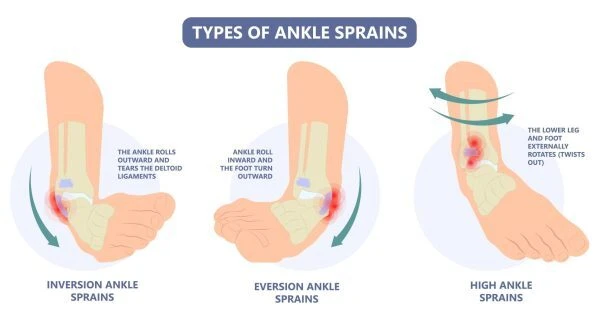
高位踝关节扭伤与一般踝关节扭伤有什么不同?
一般内翻性踝关节扭伤伤及的是踝关节外侧的韧带,会在踝关节外侧的韧带(距腓前韧带与跟腓韧带)位置产生疼痛。高位踝关节扭伤伤及的则是连结两根小腿骨、位于踝关节上方的韧带与骨间膜,疼痛位置较高,位于踝关节上方。损伤机制、疼痛位置、疼痛模式与治疗计划都不同。
高位踝关节扭伤后多久可以回到运动场?
回归运动的时间取决于损伤分级与您从事的运动。低度损伤在妥善处置下,可在 6 至 8 周时回归非接触性跑步,10 至 12 周时回归全接触性运动;较高度损伤往往需要 3 至 6 个月。关键在于渐进式的康复。回归过早常造成反覆挫折,使恢复时间拉得更长,也是再度受伤与慢性不稳的最常见原因。