
You have been treating your heel pain as plantar fasciitis for months. Stretching morning and night. Insoles in every pair of shoes. The pain has not gone. In fact, it feels worse on hard floors at home, worse without cushioning, and the morning first-step pattern that everyone talks about does not really match your experience. The pain is more like a deep bruise across the bottom of your heel, present whenever weight is on it, regardless of whether you have just stood up or have been walking for an hour.
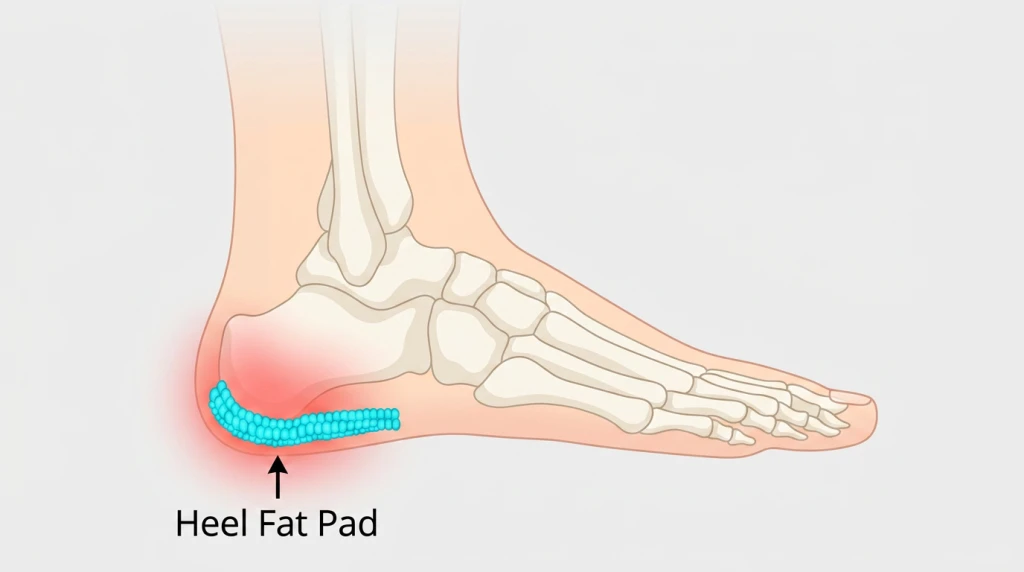
This is the recognisable picture of heel fat pad syndrome. The structure that should be cushioning your heel bone has thinned, shifted, or become inflamed, and the bone is now bearing more load than it was designed to. The condition is real, common, and frequently misdiagnosed because it presents in the same anatomical area as plantar fasciitis but follows a different mechanism. The heel fat pad is a specialised structure under the calcaneus, the heel bone, made of dense fibrous tissue arranged in chambers that contain fat globules, much like a honeycomb, designed specifically to absorb the impact of every heel strike. When the structure of the fat pad is compromised, either through age-related fat loss, repeated trauma, or a single significant impact, the cushioning function is reduced. The result is a distinctive pattern of heel pain that does not respond to standard treatments designed for the plantar fascia.
Symptoms of Heel Fat Pad Syndrome
The pain pattern in heel fat pad syndrome is typically consistent, such that it is recognisable on history alone, before any examination. The symptoms tend to develop gradually in chronic cases or appear suddenly after a specific event in acute cases.
- Deep, bruise-like pain across the underside of the heel the discomfort is usually on the outer heel, but can also spread across the entire weight-bearing surface of the heel. It is not localised to one specific point on the inside edge.
- Pain that worsens on hard surfaces tile floors at home, polished concrete in offices, and pavement walking are noticeably more uncomfortable than carpeted or cushioned surfaces.
- Pain that is worse without cushioning walking barefoot or in a pair of thin-soled shoes is significantly more painful than walking in a cushioned shoe.
- Tenderness on direct pressure under the heel pressing the centre underside of the heel reproduces the pain, often across a broader area than a single tender point.
- Pain throughout the day with weight-bearing unlike the morning first-step pattern of plantar fasciitis, the pain is generally present whenever load is on the heel and may not ease much after the first few steps of walking.
- Aching after prolonged standing extended periods on the feet produce a dull, persistent ache that takes time to settle, even at rest.
Types of Heel Fat Pad Syndrome
The clinical presentation falls into two broad patterns, and the management differs slightly between them.
Acute Fat Pad Contusion
Acute fat pad contusion arises after a specific traumatic event. The most common scenarios are jumping or landing from a height onto a hard surface, stepping awkwardly on the edge of a kerb, or accidentally landing heavily on one foot. The fat pad chambers are crushed or bruised, leading to inflammation and reduced cushioning capacity.
Pain usually appears within hours of the event and is localised to the impact area. With appropriate management, including offloading and cushioning support, most acute contusions should settle within 4 to 8 weeks.
Chronic Fat Pad Syndrome from atrophy
Chronic fat pad atrophy develops gradually over years. The fat pad thins or loses elasticity over time due to repeated impact, age-related changes, or other contributing factors. It is more commonly found in people aged 60 and above. If you have a history of long-term steroidal treatment, you may have fat pad atrophy at a much younger age.
The symptoms appear progressively over weeks or months and tend to persist longer than acute cases. Management focuses on long-term load redistribution and protection of the fat pad rather than recovery from a specific injury.
Causes of Heel Fat Pad Syndrome
Heel fat pad syndrome develops when the structural integrity of the fat pad is compromised. The fat pad is not designed to regenerate substantially once thinned, which is why prevention and protection are central to management once a problem develops.
What Causes Heel Fat Pad Syndrome?
- Repeated heel strike from running or jumping sports
- Regularly walking barefoot on hard surfaces
- Heavy landing on the heel from height
- Age-related fat pad thinning and loss of soft tissue elasticity
- Rapid and significant weight loss
- Wearing thin-soled or minimalistic shoes with no cushion
- Long-term steroid use
Who Carries a Higher Baseline Risk?
- Adults over 60, due to age-related thinning of the fat pad chambers
- Runners and recreational athletes with high cumulative mileage on hard surfaces
- People who walk barefoot at home for extended periods on tile or concrete floors
- Individuals who have lost a significant amount of body weight over a short period
- People with elevated body weight, where greater load passes through the heel with each step
- Patients with diabetes or peripheral vascular disease, where reduced tissue resilience compounds the cushioning deficit
- Those who have received multiple corticosteroid injections in the heel for previous conditions
- Persons with underlying inflammatory or autoimmune conditions that requires long-term steroid treatment
Conditions Commonly Mistaken for Heel Fat Pad Syndrome
Heel fat pad syndrome can be easily misidentified, and the distinction matters because the management approach is different for each.
Plantar fasciitis
Plantar fasciitis pain is typically sharp, localised to the inside edge of the heel where the fascia attaches, and follows a recognisable first-step morning pattern that eases with walking. Heel fat pad syndrome pain is more diffuse across the entire underside of the heel and present throughout the day with weight-bearing. Where stretching and arch support help plantar fasciitis, they have minimal effect on fat pad syndrome. Many patients carry both conditions simultaneously, which is part of why the differentiation can be missed.
Calcaneal stress fracture
A stress fracture of the heel bone produces deep heel pain that is typically more severe than fat pad syndrome and worsens significantly with any weight-bearing activity. There is often a history of a sudden increase in running or impact training. Imaging (typically MRI) is needed to confirm a stress fracture, and the management approach is fundamentally different, requiring offloading and protected weight-bearing rather than cushioning alone.
Baxter’s nerve entrapment
Baxter’s nerve entrapment produces a burning, aching, or sharp pain near the inside of the heel that can mimic plantar fasciitis or fat pad syndrome. The clue is the slight burning or electric quality of the pain, and it does not always match the load-bearing pattern of fat pad syndrome.

Treating and Preventing Heel Fat Pad Syndrome
The structural change in the fat pad is largely irreversible, particularly in chronic cases, so the goal is not to rebuild the fat pad but to protect the remaining tissue, redistribute load away from the affected area, and reduce the inflammation and discomfort that come from the deficit. The single most important principle is recognising that fat pad syndrome is not plantar fasciitis, because plans built around stretching, plantar fascia loading, or arch-only support do not address it and can prolong the frustration with no improvement.
Conservative treatment
Conservative care protects the heel and offloads the affected area, calming an acute contusion in the early phase and sustaining load redistribution in chronic cases.
- Offloading and activity modification: Reduce periods of standing and walking on hard surfaces where possible, especially in the first 1 to 2 weeks of an acute contusion, and reduce or modify high-impact activities such as running on hard surfaces in chronic cases.
- Cushioned heel cups and footwear: Cushioned heel cups or gel inserts in all daily-wear shoes, footwear with substantial heel cushioning and deep heel cups, and cushioned slippers at home rather than barefoot walking on tile or concrete all protect the heel. Avoid minimalist or zero-drop footwear, which place full load through the unprotected heel.
- Ice and anti-inflammatory measures: Ice for 15 to 20 minutes two to three times daily for the first 5 to 7 days of an acute contusion, with anti-inflammatory measures as advised by a GP where appropriate.
- Custom foot orthotics: Orthotics prescribed with specific heel cushioning and shock-absorbing materials redistribute pressure across the entire underside of the foot rather than concentrating it under the heel.
- Weight management: Managing body weight where elevated weight is adding to the load passing through the heel eases symptoms over time.
- Focused shockwave therapy and EMTT: For chronic cases that have not responded to footwear and orthotics alone, shockwave and radial pressure wave therapy can support the inflammatory and soft tissue components, and extracorporeal magnetotransduction therapy is another pain and inflammation-relieving option for selected presentations. These do not rebuild the fat pad itself.
When conservative care isn’t enough
Surgery for fat pad syndrome is rare, because there is no reliable way to surgically restore the fat pad’s cushioning structure. Most cases are managed effectively through conservative care once the diagnosis is correctly identified, and where a surgical opinion is genuinely warranted, a referral to an orthopaedic surgeon is arranged.

Have Your Heel Fat Pad Syndrome Managed at Straits Podiatry
Heel fat pad syndrome is one of the most under-recognised causes of persistent heel pain. Patients often arrive having been treated for plantar fasciitis for many months without improvement, frustrated and unsure why nothing has helped. The first step in management is correctly identifying that fat pad syndrome is what is actually present, which involves carefully distinguishing it from plantar fasciitis, calcaneal stress fracture, Baxter’s nerve entrapment, and other potential contributors to heel pain.
At Straits Podiatry, this assessment focuses on the precise pain pattern, the response to specific provocation tests, the condition of the fat pad on examination, and any contributing factors such as footwear, activity history, and body weight changes. From that assessment, a management plan is built around the specific presentation and severity. This may include custom foot orthotics designed specifically to cushion the heel and redistribute pressure away from the affected area, footwear guidance to ensure daily-wear shoes provide adequate protection, extracorporeal shockwave therapy or radial pressure wave therapy for chronic cases.
If you are suffering from heel pain when walking, speak with our team or book a consultation for an assessment and a tailored approach to manage your heel fat pad syndrome.
Frequently Asked Questions About Heel Fat Pad Syndrome
How is heel fat pad syndrome different from plantar fasciitis?
Plantar fasciitis pain is typically sharp and localised to the inside edge of the heel where the plantar fascia attaches to the heel bone, and it follows a recognisable first-step morning pattern that eases after walking. Heel fat pad syndrome pain is more diffuse across the entire underside of the heel, feels deeper and more like a bruise, is worse on hard surfaces and without cushioning, and persists throughout the day rather than easing after the first few steps. Stretching and arch support, which help plantar fasciitis, generally have minimal effect on fat pad syndrome. The two conditions can coexist, and accurate diagnosis is what determines whether the treatment plan will work.
Can the heel fat pad regenerate or rebuild?
The fat pad’s structural chambers and the fibrous tissue that holds them in place do not reliably regenerate once damaged or thinned. This is why management focuses on protecting the remaining tissue and redistributing load rather than attempting to rebuild the cushioning. With the right combination of footwear, custom orthotics, and activity modification, most patients can return to comfortable daily activity, even if the fat pad itself does not recover its previous thickness.
Will weight loss make heel fat pad syndrome worse?
Significant or rapid weight loss can reduce the fat content of the heel pad alongside other body fat stores, which sometimes contributes to fat pad atrophy. This does not mean that healthy weight management should be avoided, particularly if elevated weight is itself contributing to heel load. The aim is gradual, sustainable weight management combined with protective footwear and orthotic support during and after the weight loss period to compensate for any fat pad thinning that may occur.
How long does heel fat pad syndrome take to settle?
Acute fat pad contusion typically settles within 4 to 8 weeks of consistent management with cushioning, offloading, and activity modification. Chronic fat pad syndrome takes longer because the underlying structural change is not reversed by treatment. Most patients with chronic fat pad syndrome see meaningful symptom improvement within 6 to 12 weeks of starting a structured plan with appropriate orthotics and footwear, but ongoing protection of the heel is needed long-term to prevent recurrence.
When should I see a podiatrist for heel fat pad syndrome?
If you have been treating heel pain as plantar fasciitis for more than 6 to 8 weeks without improvement, particularly if your pain pattern does not match the typical first-step morning pattern, that is a reasonable point to seek an assessment. Other indicators include heel pain that is worse without cushioning, heel pain following a specific impact or trauma, persistent heel pain after significant weight loss, or heel pain in adults over 60 with no other clear cause. A podiatry assessment can clarify whether fat pad syndrome is the correct diagnosis and build a management plan specific to it.